Most Affordable Care
We believe in making treatment accessible at the lowest possible cost — so more people can get the care they deserve. And yes, it actually works.
A Treatment That Finally Works
You’ve tried everything but nothing sticks. It’s time to work with your biology, not fight against it.
Bolt provides safe, effective GLP-1 medications so you can regain your self-confidence & live life in color. No more going through the day-to-day grayness. This time it’s sustainable.
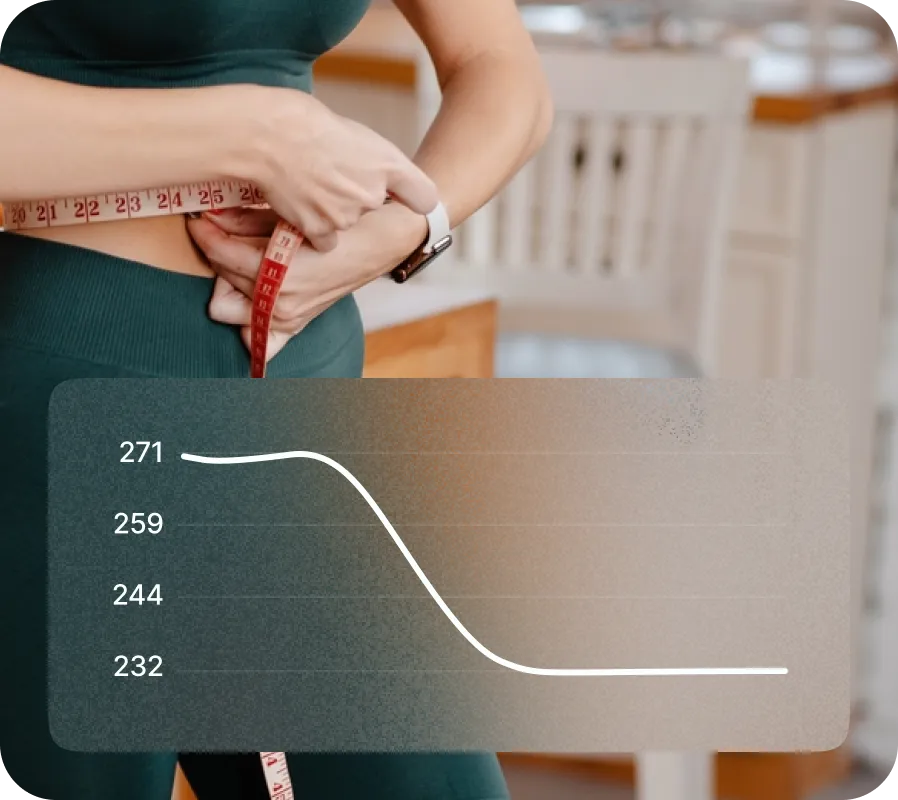
Sustainable Weight Loss
Forget crash diets and quick fixes. With Bolt, you lose weight steadily — and stay there.
No more bouncing back. This is long-term change.










.svg)
.avif)


.webp)
.webp)
.webp)
.webp)